
Hip Impingement? Not just a pinch!
Hip impingement is a general term for pinching or positional sensitivity to hip flexion(knee towards chest). More often, this is diagnosed as femoroacetabular impingement(FAI), which is an intra-articular(joint) condition resulting in mechanical compression of the hip joint.
A little anatomy review, the hip is ball-and-socket joint. The acetabulum is the socket and the femoral head is the ball. The joint is lined with cartilage, which promotes a smooth, low friction surface for joint motion. The structure of the joint provides quite a bit of stability, but the fibrocartilaginous labrum improves this by creating a gasket-like seal.
Through imaging, impingement can be further classified as a cam lesion, pincer, or combined. A cam lesion involves a dyfunctional femoral head that is not quite as round as it should be, at times resulting in bone spur/osteophyte formation and degradation of the acetabular cartilage. A pincer involves a larger than normal socket. This can result in degradation of the labrum and cartilage. Combined impingement involves both a cam lesion and pincer.
In October of 2015, Nikolaos V. Bardakos published a journal article in The Journal of Hip Preservation Surgery outlining the evaluation, imaging, and treatment(mostly surgical) of numerous varying types of hip impingement. He described ischiofemoral, subspine, iliopsoas, trochanteric-pelvic, and pectineofoveal impingements. Many of these involve slight variances from the norm regarding bony structures, which are not addressed in the most common surgeries to improve FAI. Additionally, he extrapolated how most of these types of hip impingement actually involve soft tissue structures.
In my clinical experience, I’ve seen many patients successfully return to activity without symptoms with and without surgery. Unfortunately, I have also seen patients with very little improvement following arthroscopic surgery to address FAI. In many instances, the individual has developed compensatory movement patterns resulting in dysfunctions above and below the hip. Don’t get me wrong. I am not the physical therapist that talks everyone out of surgery. More so, I think a thorough evaluation and investigation of the aforementioned sources of hip pain/impingement are essential.
Many times, the anterior structures of the hip are painful due to poor hip/pelvic stability. Look at the picture below…

The left photo shows the pelvic in an anterior tilt while the right shows a posterior tilt. What if this person goes into a squat? Without going into too much detail, the femur(thigh) would approximate with the pelvis much earlier with the person on the left right? So, spine position and core stabilization plays a large role! Additionally, improving the extensibility of the hip joint and strengthening the glutes and hip rotators to better stabilize the femur in the acetabulum can help. Exercises such as the (soap box moment) over-recommended clamshell, banded bridge march, Jane Fonda(side leg raise), single leg squat, and training your core with a neutral spine are commonly recommended. Below, you will see some pretty horrible illustrations of these exercises. Don’t do #3…not sure what is going on there.
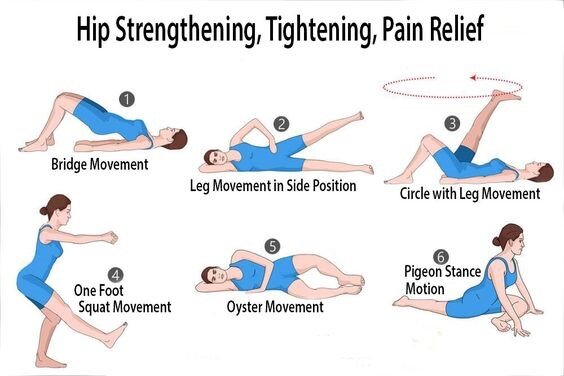
Now, these are just general exercises. As mentioned previously, a thorough evaluation would provide better guidance and exercise recommendations.